 Encyclopædia Neurochirurgica
Encyclopædia Neurochirurgica
 PITUITARY ADENOMAS
PITUITARY ADENOMAS


4. Diagnosis
Diagnosis is based on clinical symptoms complemented with other tests, on imaging (incidental finding) or on ophthalmic symptoms.
*4.1 Clinical Features
Prolactinoma
For more details, readers may refer to the articles of the following consensuses : Casanueva clin endocrinol 2006, Brue Ann Endo 2007, Melmed JCEM2011 [1].
Two Presentations:
![]() The Classic Microadenoma (<10mm) or "small" macroprolactinoma of the young woman results to an amenorrhea (sometimes spanio- or oligomenorrhea) -galactorrhoea (spontaneous or induced) syndrome, with decreased libido and infertility, headaches and weight gain. This is a well circumscribed tumor that is rarely invasive. The problem is the restoration of fertility.
The Classic Microadenoma (<10mm) or "small" macroprolactinoma of the young woman results to an amenorrhea (sometimes spanio- or oligomenorrhea) -galactorrhoea (spontaneous or induced) syndrome, with decreased libido and infertility, headaches and weight gain. This is a well circumscribed tumor that is rarely invasive. The problem is the restoration of fertility.![]() Prolactinoma in males is of late onset in the 50s by a mass effect (tumoral syndrome) with visual affection (bitemporal hemianopsia is pathognomonic). Decreased libido with erectile dysfunction is the norm, but leads to belated consultation. Gynecomastia may exists but galactorrhoea is rare. PRLomas in males are macroadenomas, not because of their late onset but because of their more agressive character25,74. MRI reveals a macroadenoma sometimes very large (Figure 3).
Prolactinoma in males is of late onset in the 50s by a mass effect (tumoral syndrome) with visual affection (bitemporal hemianopsia is pathognomonic). Decreased libido with erectile dysfunction is the norm, but leads to belated consultation. Gynecomastia may exists but galactorrhoea is rare. PRLomas in males are macroadenomas, not because of their late onset but because of their more agressive character25,74. MRI reveals a macroadenoma sometimes very large (Figure 3).
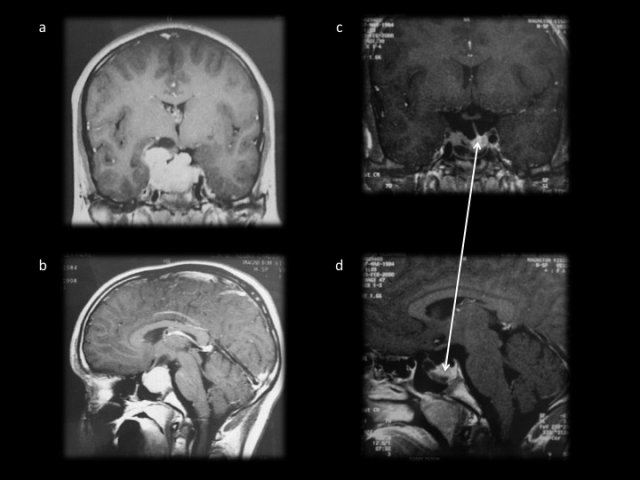
- Figure 3 : a et b coupes coronale et sagittale d’un macroprolactinome. c et d : résultat après un an de traitement par dostinex. La fonte tumorale est spectaculaire avec une hypophyse parfaitement fonctionnelle visible à gauche en intrasellaire (flèche blanche). La récupération visuelle a été totale.
Somatotropic Adenoma
For more details, readers may refer to the articles of the french (Chanson Ann Endo 2009) and American (Melmed JCEM 2009) consensuses on acromegaly [2].
Clinically, acromegaly results in the classic dysmorphic syndrome associating increase in the nasal pyramid, bony prominences including eyebrows, prognathism, an increase in the size of the hands and feet (figure4).
Carpal tunnel syndrome can be the presenting picture. Headache is common, as well as pungent very distressing night sweats. Sleep Apnoea Syndrome (SAS) is the norm and ought to be screened. It can be associated with chronic fatigue. A depressive reaction is also common. The morbidities of this disease are cardiac (hypertension and hypertrophic cardiomyopathy), endocrine (glucose intolerance or diabetes) and rheumatologic affecting large joints (shoulder, wrist, knee, hip) and spine. Finally goiter is common, as well as polyps of colon justifying systematic colonoscopy in the initial work up. The increased incidence of colon cancer, as well as thyroid in acromegaly should be emphasized.
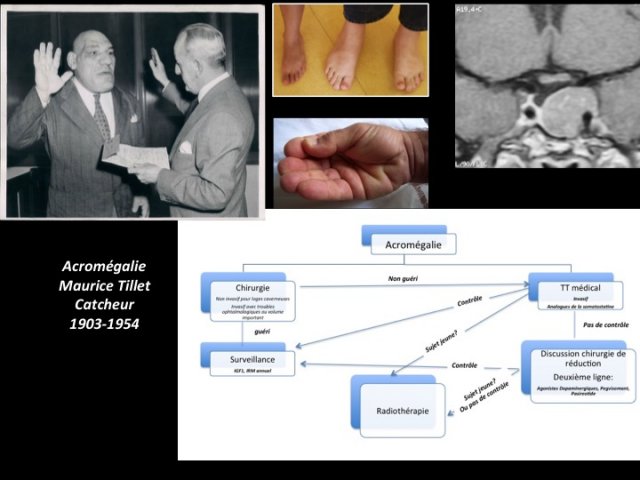
- Figure 4 : photos du syndrome dysmorphique de l’acromégalie. L’algorithme du bas résume la prise en charge actuelle de l’acromégalie où la priorité est donnée à la chirurgie autant que faire se peut.
Corticotropic Adenoma
We consider Cushing’s disease with ACTH dependent hypercortisolism due to a pituitary adenoma rather Cushing’s syndrome with ACTH-independent Hypercorticism. This paragraph summarizes published articles of recent consensuses French Health Authority Report, Biller JCEM 2008) [3].
The clinical signs (figure 5) reflect a state hypercatabolism (skin: large and purple stretch marks, ecchymoses, vascular fragility ; proximal muscle atrophy ; bone: osteoporosis) with facial-truncal fat distribution (abdominal obesity with buffalo hump or Buffalo Neck at the base of the neck).
In children there is a decrease in the growth curve, with a paradoxical weight gain. Morbidities are severe with hypertension, diabetes, osteoporosis and severe immunosuppression and in addition to physical disfigurement. Psychiatric or psychological effects are common.
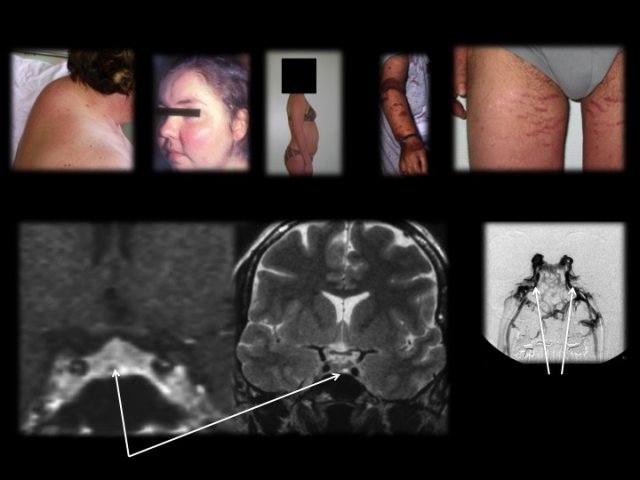
- Figure 5 : Photos du syndrome dysmorphique du Cushing. L’adénome est de type micro (flèche) parfois invisible sur l’IRM. En cas de négativité de l’IRM, un cathétérisme des sinus pétreux inférieurs est réalisé, le radiologue positionnant les micro-cathéters dans la partie verticale des sinus (flèches).
Thyrotropic Adenoma
Thyrotropic adenomas (secreting excess TSH) are rare, representing less than 1% of pituitary adenomas.
The clinical picture is that of a thyrotoxicosis with nervousness, weight loss and cardiovascular disorders (hypertension, palpitations, arrhythmias) associated with a tumor syndrome (headache, visual disturbances) in about a quarter of cases. Amenorrhoea is common (25%) so is goiter with a similar frequency of occurrence
[4].
Non-Secreting Or Nonfunctioning Pituitary Adenomas (Gonadotrophin And "Silent" Adenomas)
The consensus of the French Society of Endocrinology is to be published in the Annals of Endocrinology and a chapter in the EMC is dedicated to this type of tumor (Raverot et al. EMC 2014) [5].
Most pituitary adenomas do not secrete active hormones and present with a tumor syndrome (mass effect) or discovered incidentally. In fact, the secretion of FSH, LH or α subunit (these "gonadotropins" are glycoproteins composed of two subunits : α andβ) is rarely responsible for manifestations of ovarian hyperstimulation (cysts) or testicular hypertrophy.
Clinically, visual disturbances are presenting features (bitemporal hemianopia is pathognomonic, is often asymmetrical but frequently associated with a decrease in visual acuity (uni- or bilateral)) ; an anterior pituitary gonadotropin insufficiency is common (posterior pituitary insufficiency is exceptional) and headache with no special characteristics.
Cases of incidentalomas are on an increase.
Atypical Pituitary Adenomas And Carcinomas
There is no clinical feature specific of these adenomas apart from their high recurrence and resistant to conventional therapy.
Pituitary Apoplexy
Pituitary apoplexy is a clinical syndrome characterized by sudden headache (true differential diagnosis of subarachnoid hemorrhage), ophthalmological affection of variable severity (decreased visual acuity, visual field disturbances, oculomotor palsy) and / or anterior and posterior-pituitary failure with hyponatremia. The setting is that of emergency sometimes difficult to manage.
The pathophysiology is that of either an infarction, or an intra-adenomatous hemorrhage with sudden increase in the volume and intra-sellar pressure.
Pituitary apoplexy can occur as the initial presentation of the tumor or as a complication of the course of the pituitary adenoma. The incidence of apoplexy is low (2-7% of all adenomas). Contributing factors include 60:
- Cardiovascular risks: hypertension, coronary heart surgery (pressure variations and use of anticoagulants)
- Iatrogenic: antiplatelet drugs, anticoagulants, dynamic hormone tests during work up for pituitary adenoma (GHRH, CRH, TSH), treatment with dopamine agonists or oestrogenes
- Pregnancy
- Head trauma
- Pituitary radiation therapy? They occur more frequently between the 5th to 6th decades and with a slight male predominance.